
After over 40 years of practice in this fascinating field some basic principles remain, but there are also new concepts and technologies to evaluate and incorporate into our treatment regimes. Anatomy remains the foundation and “basic science” of all we do. In this blog, we will look at trends in blepharoplasty, facelift, and skin resurfacing.
займ онлайн на карту круглосуточно
Upper blepharoplasty has probably changed the least of these procedures. We still use the same basic incisions. With a better understanding of the importance of fullness for youthful beauty, we rarely remove fat from the middle-fat pocket both to preserve the youthful look and avoid an operated “A” shape to the upper lids. However, there are numerous newer techniques to change the lid fold.
Lower blepharoplasty has also changed with a recognition of the role played by cheek descent with age in creating an undesirable cheek lid contour. Our treatment options include mid-facelift, fat transposition, or fillers to repair this deformity. Early on we almost always approached the lower lid with a skin muscle flap sub-ciliary incision but as the transconjunctival approach became popular it became our technique of choice.
In recent years, however, we find ourselves performing more skin muscle flap procedures again to address muscle laxity and more precisely transpose fat and lift the SOOF. There is also a renewed focus on supporting the lower lid with various canthoplasty and canthopexy techniques. Finally, some of the factional lasers provide excellent nonsurgical treatments.
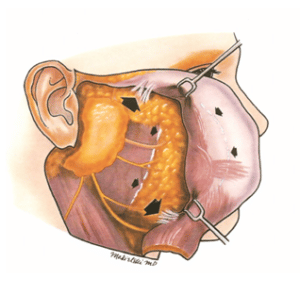
Our facelift technique has evolved continuously over the last 40 years. We originally performed a smaller SMAS flap procedure or simple plication in some cases. We advised our patients they would need a “Tuck-up” in a few years and they did! The two biggest conceptual changes over the years have been to understand the need to release the facial ligaments and to address the volume loss patients sustained with age. Our current technique is very individualized, and a combination of procedures advocated by others.
Resurfacing is the area where we have seen the most change. 40 years ago, we performed mainly phenol peels- mostly of the Gordon Baker variety but with some TCA peels also. Beginning in the 1990’s we began to perform CO2 laser resurfacing. Initial results were good but problems particularly with delayed hypopigmentation caused many to avoid the procedure. The last decades have seen many innovations.
The fractionated CO2 first appeared and rapidly became the “gold standard” for facial rejuvenation. Erbium lasers became more common. Various non-ablative approaches appeared also. Modern resurfacing lasers are highly tunable in both fractionated and full-field modes. We are currently excited by the Halo which can provide almost ablative results with a relatively low downtime procedure.